Zika virus
![]() 3 Min
3 Min
![]() 3 Min
3 Min
![]() 3 Min
3 Min
 Zika virus is a mosquito borne infection transmitted by the female Aedes mosquito. Zika is an emerging viral infection that was first identified in Uganda in 1947.1
Zika virus is a mosquito borne infection transmitted by the female Aedes mosquito. Zika is an emerging viral infection that was first identified in Uganda in 1947.1
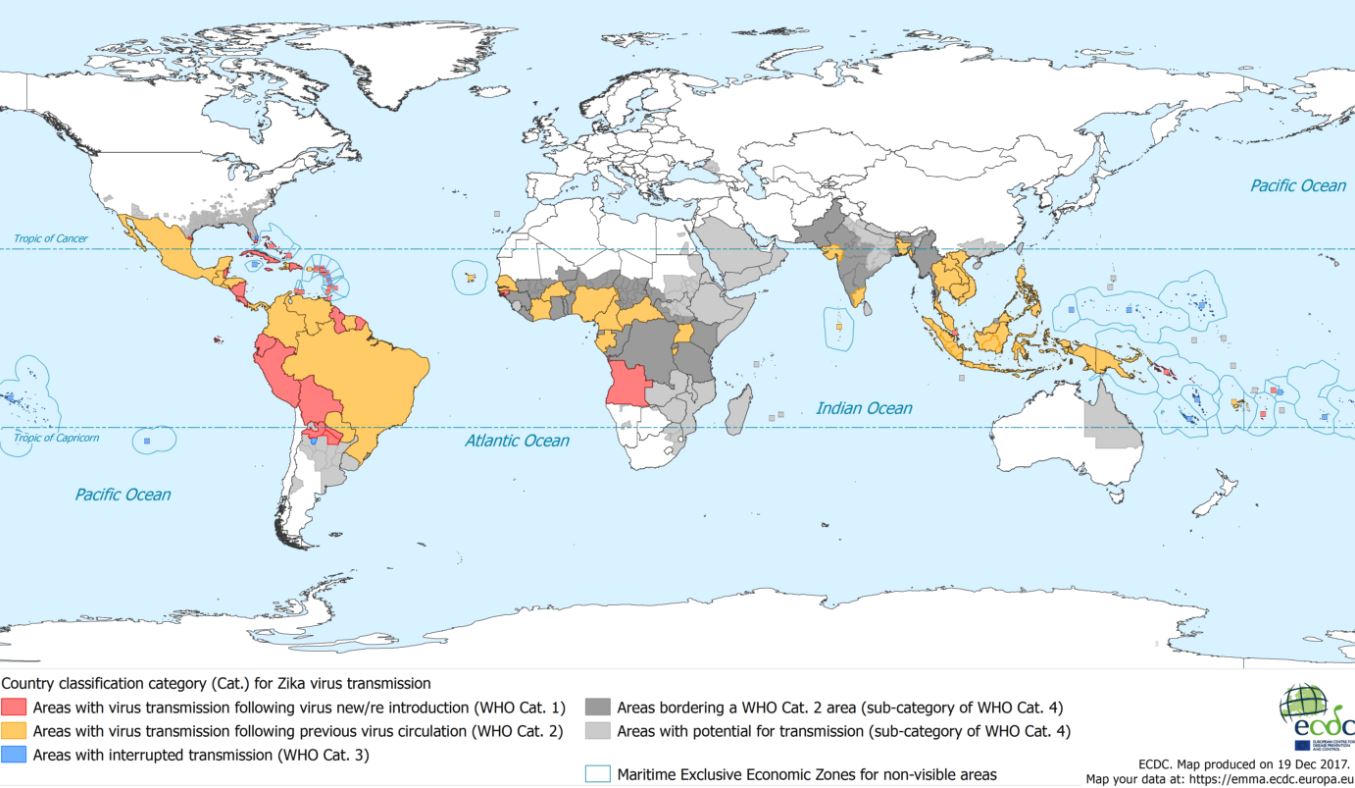
Outbreaks of the virus have since been reported in Africa, the Americas, Asia and the Pacific. Infection with the virus is becoming increasingly prevalent in Central and Southern America, the Caribbean and Pacific islands.
The infection has been linked with congenital defects in children born to mothers infected with the virus.
Zika virus is transmitted by the bite of an infected female Aedes mosquito. The Aedes aegypti species is most commonly associated with the spread of Zika virus but other Aedes species can also transmit the infection.
Zika virus has been reported from countries in Africa, Asia, Australasia and the Pacific, Central and South America, the Caribbean and North America.
Public Health England provides an A-Z list of countries showing the Zika virus risk rating which can be found at https://www.gov.uk/guidance/zika-virus-country-specific-risk
Symptoms typically develop within 3 to 12 days after being bitten,1 although the incubation period can be shorter in some people.
Aedes mosquitos mostly bite during the day and around dusk and dawn as opposed to malaria transmitting mosquitos which bite at night between dawn and dusk.
Zika virus is not contagious. Theoretically individuals exposed to infected blood could be at risk especially if there is blood to blood contact or penetrating injury, such as a needle stick injury.1
The majority of people who are infected with Zika virus are asymptomatic. For those who develop symptoms they are generally mild and short lived, lasting only about 2 to 7 days.
Typical symptoms of Zika virus are2:
Other less common symptoms include anorexia, diarrhoea, constipation, abdominal pain and dizziness.1
The symptoms associated with Zika virus are similar to dengue or chikungunya which are transmitted by the same mosquito species and are infections that are frequently co-circulating in areas of the world where Zika is present.
Guillain-Barré syndrome, a potentially fatal neuropathic condition that leads to weakness and loss of sensation in the arms and legs, has been shown to be triggered by Zika virus infections5.
For most patients Zika virus only causes mild and short-lived symptoms. However, Zika has a possible association with congenital malformations.
A 20-fold increase in the incidence of microcephaly in Brazil has led to the Brazilian Ministry of Health declaring a public health emergency. Current evidence suggests that Zika virus can pass between a mother and unborn child (placental transmission). A possible link between the recent outbreak of Zika virus and increased incidence of microcephaly has been suggested.3
Microcephaly is a birth defect where the baby's head is smaller than expected when compared to babies of the same sex and age. The condition is often associated with a smaller brain that might not have developed correctly.
Because of the potential link between Zika virus and microcephaly, women who are either pregnant or trying to conceive are advised to avoid travelling to areas where Zika virus is prevalent. Where travel is unavoidable they should be urged to be particularly vigilant in preventing mosquito bites. They should also be advised to seek medical attention if they experience any feverish illness either whilst travelling or when they return home.
Evidence is now available which seems to confirm suspicions that Zika virus may also be sexually transmitted.
Zika virus has been detected in semen two months after clinical symptoms presented. It is as yet unknown if the virus can persist for longer than two months.
A growing number of probable sexually transmitted cases of Zika infection (male to female) have been reported.4
A published case report from France has described transmission from an asymptomatic man to his female partner between 21 and 30 days after return from a Zika endemic area.
Patient Advice for travel to high to moderate risk areas
Women of childbearing age
Women of child bearing age should use contraception during travel and for 8 weeks afterwards to avoid the risk of Zika virus in an unplanned pregnancy.
Men
Men should use condoms during travel to avoid the risk of sexual transmission of Zika virus and for 6 months after return even in the absence of symptoms and also for the duration of their partner(s) pregnancy.
Pregnant women
Pregnant women should postpone non-essential travel to high risk areas until after pregnancy. They should consider postponing non-essential travel to moderate risk areas.
If they do have to travel then strict bite avoidance measures are required and barrier methods of contraception are recommended to prevent sexual transmission. They should seek advice from their GP or midwife on return, even if they have not been unwell.
There is currently no vaccine or drug that will prevent infection with Zika virus.
Travellers should be advised that bite avoidance is the only method for preventing infection with Zika virus.
Suitable advice for travellers regarding bite avoidance would include:
There is no antiviral treatment for Zika virus; standard treatment involves symptomatic relief, adequate fluid intake and rest.
Pharmacists are ideally placed to advise patients of the possible risks of infection whilst travelling abroad, including Zika virus. For a detailed account of travel risk assessment read our Pharmacy Excellence on Travel Risk Assessment.
An awareness of the specific risks for individual patients and areas of the world ensures that pharmacists are able to provide accurate, timley and up to date information.